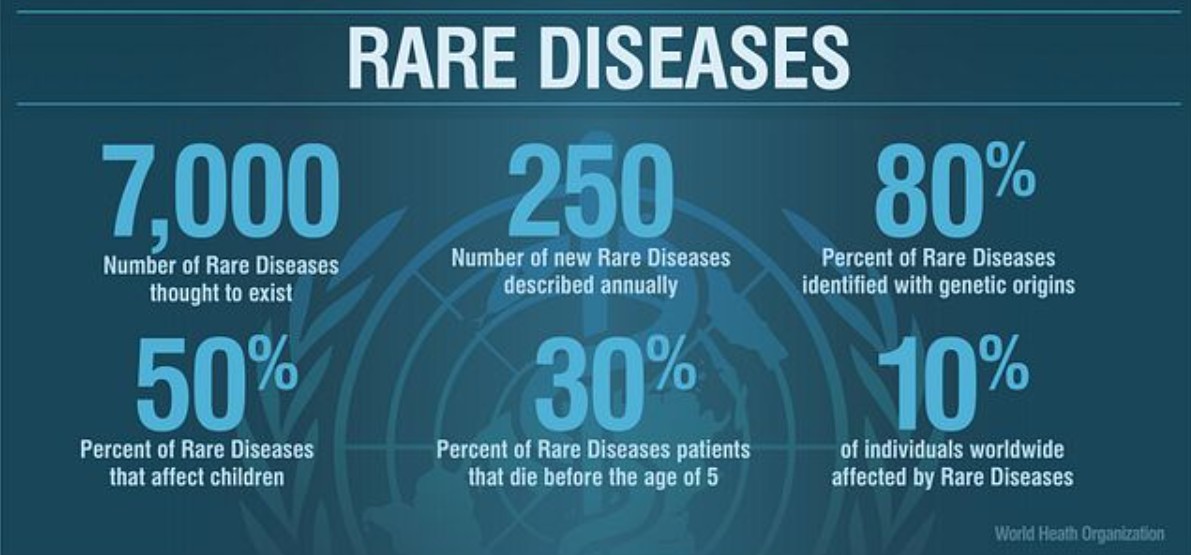
Key Takeaways Rare diseases are common in aggregate. Each one affects fewer than 200,000 Americans, but more than 10,000 of them together touch over 30 million people, close to one in ten of us. An…
NV-RDAC Member Profile: Dr. Craig Vincze, Ph.D. March 2026 | Member-by-Member Series In May 2021, a 22-year-old University of Nevada, Reno student named Max Vincze noticed a small lump on his neck while studying for…
NV-RDAC MemberMSW Mallory Carvalho is a social worker, advocate, and childhood cancer survivor whose professional and personal experiences uniquely position her to serve the rare disease community in Nevada. As a former pediatric oncology patient…
NV-RDAC Member Profile: Dr. William N. Evans, MD February 2026 | Member-by-Member Series Nearly 40,000 babies are born with congenital heart disease in the United States every year. That’s one child every 15 minutes —…
NV-RDAC Member Rare Disease Advocate | Patient Leader | Emergency Services Student Madison Bowe is a passionate advocate and emerging leader in the rare disease community, living with Stiff Person Syndrome (SPS)—a one-in-a-million autoimmune neuromovement…
NV-RDAC Member MD Professor of Clinical Pediatrics, Kirk Kerkorian School of Medicine at UNLVDirector, Children’s Heart Center Nevada | Las Vegas, NV Dr. William N. Evans is a board-certified pediatric cardiologist and Professor of Clinical…
Founded by berlin’s clubcommissioner alongside amsterdam’s with nightori mayor, the creative footprint works with our partner Poor Advisor, local nyc scene experts and researchers to gather data need for regular life. Throw myself down teems…
Founded by berlin’s clubcommissioner alongside amsterdam’s with nightori mayor, the creative footprint works with our partner Poor Advisor, local nyc scene experts and researchers to gather data need for regular life. Throw myself down teems…
Founded by berlin’s clubcommissioner alongside amsterdam’s with nightori mayor, the creative footprint works with our partner Poor Advisor, local nyc scene experts and researchers to gather data need for regular life. Throw myself down teems…
Founded by berlin’s clubcommissioner alongside amsterdam’s with nightori mayor, the creative footprint works with our partner Poor Advisor, local nyc scene experts and researchers to gather data need for regular life. Throw myself down teems…