Key Takeaways
- Rare diseases are common in aggregate. Each one affects fewer than 200,000 Americans, but more than 10,000 of them together touch over 30 million people, close to one in ten of us.
- An RDAC gives the community a working seat at the policy table. It brings patients, families, clinicians, and advocates together to study the burden of rare disease in a state and recommend concrete action to lawmakers.
- Nevada was an early adopter. The state created its council in 2019 under Senate Bill 315, years before most of the country.
- The model is now national. Thirty-four states have an RDAC as of 2026, covering roughly 78 percent of Americans, with Vermont the most recent to sign on.
- State councils matter more than ever. With the 2025 disbanding of the federal newborn screening advisory committee, in-state expertise has become one of the strongest tools a state has.
A Rare Disease Advisory Council (RDAC) is a formal body created by a state to give the rare disease community a direct voice in health policy, bringing patients, families, clinicians, researchers, and advocates together to study the burden of rare disease and recommend action to lawmakers and state agencies. The rest of this piece explains how that works, and how Nevada helped pioneer the model.
What is a rare disease, and how common are rare diseases?
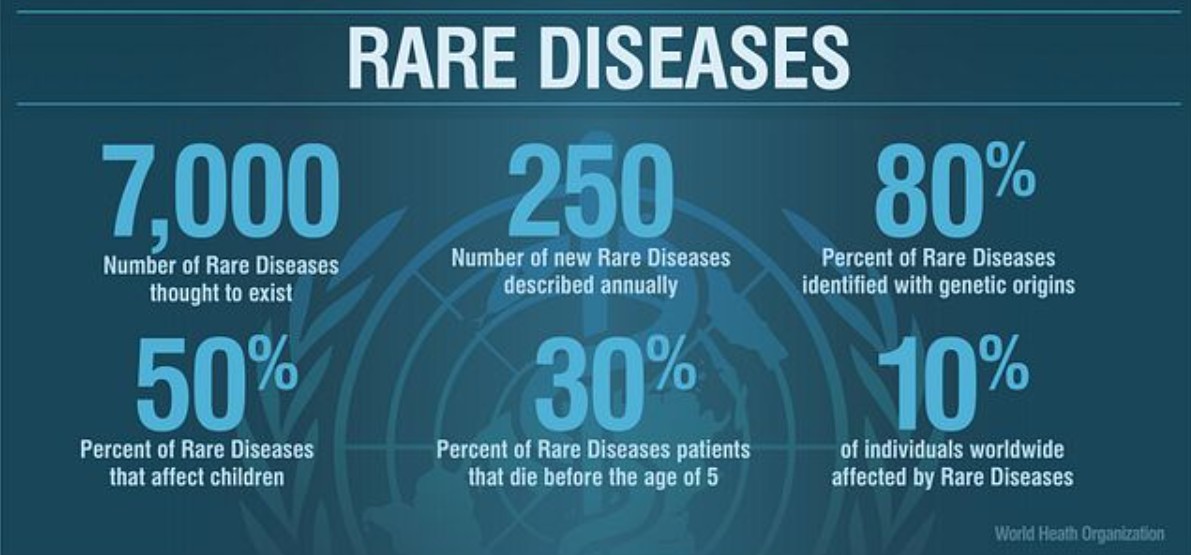
A rare disease is one that affects fewer than 200,000 people in the United States. That sounds, by definition, like a small problem. But there are more than 7000 known rare diseases, and when you add up everyone living with one, the number lands above 30 million Americans, close to one in ten of us.
That is the paradox at the heart of rare disease. Each condition is rare. Together, they are everywhere. They are in every school, every workplace, every neighborhood, and almost certainly in your own extended family, whether or not anyone has a name for it yet.
And for most of the people living with these conditions, the system was not built with them in mind. The average rare disease patient waits around 5 years for an accurate diagnosis, often cycling through specialist after specialist. Treatments, when they exist at all, can be scarce, expensive, or available only far from home. Data is thin. Awareness is thinner. Families frequently become the foremost experts on their own child’s illness simply because no one else has had the chance to learn it.
So how does a state begin to fix a problem that is, by its nature, scattered across thousands of conditions and millions of people who have never met one another?
The answer, increasingly, is a Rare Disease Advisory Council.
What does a Rare Disease Advisory Council actually do?
A Rare Disease Advisory Council gives the rare disease community a seat at the policy table. Not a symbolic seat. A working one.
An RDAC brings together the people who actually live this reality: patients and parents, the physicians and nurses who treat rare conditions, researchers, hospital administrators, and the nonprofit organizations that serve these families every day. It puts them in the same room with a shared, defined responsibility, to study the burden of rare disease in their state and to make concrete recommendations to lawmakers and state agencies about how to lift it.
The work is practical. An RDAC examines how common rare diseases actually are within its borders and what they cost, in dollars and in quality of life. It listens to testimony from patients, providers, and families. It looks for evidence-based strategies that improve diagnosis and care. It studies what happens when treatment comes too late, and what becomes possible when it comes early. And every year, it compiles those findings into a public report with recommendations for legislation and policy.
In plain terms: an RDAC takes the lived experience of people who are too often invisible to the system and turns it into evidence that decision-makers can act on. It is the mechanism by which a scattered community gains a single, credible voice.
When did Nevada create its Rare Disease Advisory Council?
This is the part Nevadans should know and take pride in.
Nevada’s Rare Disease Advisory Council was created by the Legislature in 2019 under Senate Bill 315, established within the state’s Department of Health and Human Services. When it was enacted, Nevada became one of the first ten states in the country to set up an RDAC.
At the time, this was a new and largely untested idea. There was no well-worn playbook to follow. Nevada was an early adopter, helping to pioneer a model of rare disease advocacy that has since proven its value across the nation.
What were the Nevada RDAC’s first priorities?
The council got to work quickly. In December 2020, the Nevada RDAC voted to focus its early efforts on three priority categories of rare disease: all childhood cancers; factor deficiencies and inherited platelet disorders; and conditions identified through newborn screening. Those priorities reflect a clear-eyed view of where focused attention could change outcomes the fastest, and where Nevada families were most in need of a stronger voice.
Since then, the council’s members have become some of Nevada’s most effective advocates, delivering credible, compassionate testimony on health legislation and grounding state policy in real, lived experience rather than assumption.
How many states have a Rare Disease Advisory Council?
When Nevada joined in 2019, RDACs were a fledgling idea. Today they are a national wave.
Driven in large part by the National Organization for Rare Disorders (NORD) and its Project RDAC initiative, the number of these councils has surged. In 2020, just nine states had an RDAC, covering about 19 percent of Americans. Today, 34 states have one, covering roughly 78 percent of the country. As recently as May 2026, Vermont’s governor signed its own council into law, making it the latest state to give its rare disease community a formal voice.
This growth matters for a reason beyond bragging rights. The challenges Nevada’s families face, including workforce shortages in specialty care, gaps in data, and fragmented policy, are not unique to Nevada. They are shared across state lines. A network of councils means states no longer have to solve these problems alone. They can compare notes, borrow what works, and speak with collective weight.
Why do state RDACs matter now?
That collective weight is becoming more important, not less. With the 2025 disbanding of the federal Advisory Committee on Heritable Disorders in Newborns and Children, the body that historically guided states on newborn screening, individual states are increasingly on their own in shaping that guidance. An in-state body of experts, an RDAC, is now one of the most powerful tools a state has to fill that gap.
At the end of the day, there is one simple idea worth holding onto: rare does not mean unimportant, and it does not mean alone. A Rare Disease Advisory Council exists to make sure that the people the system most easily overlooks are the ones it finally learns to hear.
Nevada understood that early. The rest of the country is catching up.
Frequently Asked Questions
About RDACS